
Introduction
The ADASS mental health network has long recognised the key role of mental health social workers in achieving excellence in person centred discharge. Partners in Health and Care commissioned the Social Care and Health Collaborative to develop this practical guidance which draws on extensive engagement with front line teams, statutory guidance and mental health discharge operational models that are working well across the country.
Mental health discharge: national context
Across the country, the challenges with mental health discharge processes are multifaceted and can be attributed to several systemic issues. These issues were clearly identified during December 2022 to March 2023 as a result of the NHS England Discharge Challenge for Mental Health and Community Service. The key themes emerging through this work are summarised.
To address these challenges, workforce development, service integration, collaborative partnership working, and comprehensive collaborative discharge planning are essential. Ensuring that patients have access to a continuum of care, from inpatient treatment to community support, is crucial for improving outcomes and reducing the likelihood of readmission.
Increased demand/acuity
Linked in part to COVID-19 and the cost of living crisis, as well as increases in specific complex cohorts.
Lack of suitable housing or accommodation
Linked to commissioners' and clinicians' trust in supported housing.
More patients being admitted at point of crisis
Resulting in more complex needs and longer length of stay.
High staff turnover and vacancies
Makes the implementation of action points difficult.
A culture of risk aversion
Meaning patients are admitted without therapeutic requirement and a reluctance to discharge without care packages.
Community capacity - increasing caseloads
Leading to a lack of capacity in teams meeting the person's needs on discharge and preventing relapses.
Inconsistent discharge planning processes
From point of admission, including lack of consistency in recording reasons for delay.
Funding disputes between NHS and councils
Disputes for support package or specialist accommodation, particularly where individuals are 'out of area'.
Information and data
Enabling more robust data that can be shared across systems to understand reasons for delays.
Statutory mental health hospital discharge guidance
On 26 January 2024, the Department of Health and Social Care published Statutory guidance: discharge from mental health inpatient settings. The guidance provides eight key principles for how NHS bodies (including NHS trusts, NHS foundation trusts and integrated care boards (ICBs)) and councils should work together for effective discharge planning from all mental health inpatient services:
- Principle 1: Individuals should be regarded as partners in their own care throughout the discharge process and their choice and autonomy should be respected.
- Principle 2: Carers should be involved in the discharge process as early as possible.
- Principle 3: Discharge planning should start on admission or before and should take place throughout the time the person is in hospital.
- Principle 4: Health and council social care partners should support people to be discharged in a timely and safe way as soon as they are clinically ready to leave hospital.
- Principle 5: There should be ongoing communication between hospital teams and community services involved in onward care during the admission and post-discharge.
- Principle 6: Information should be shared effectively across relevant health and care teams and organisations across the system to support the best outcomes for the person.
- Principle 7: Local areas should build an infrastructure that supports safe and timely discharge, ensuring the right individualised support can be provided post-discharge.
- Principle 8: Funding mechanisms for discharge should be agreed to achieve the best outcomes for people and their chosen carers and should align with existing statutory duties.
These eight key principles are woven throughout the following framework for achieving excellence in mental health discharge.
A framework for achieving excellence in mental health discharge
This framework has been developed through extensive engagement with front line teams, drawing on best practice guidance and mental health discharge operational models that are working well across the country. The premise of the framework is based on the discharge to assess (D2A) model.
This framework includes people with a learning disabilities and or autism and should be implemented alongside the recommendations of the five key elements for discharge and the 'Cultures of standards of care for mental health inpatient support.'
The framework for achieving excellence in mental health discharge consists of three main components:
- essential system partnerships
- language and frameworks
- pathways, based on the discharge to assess (D2A) model.
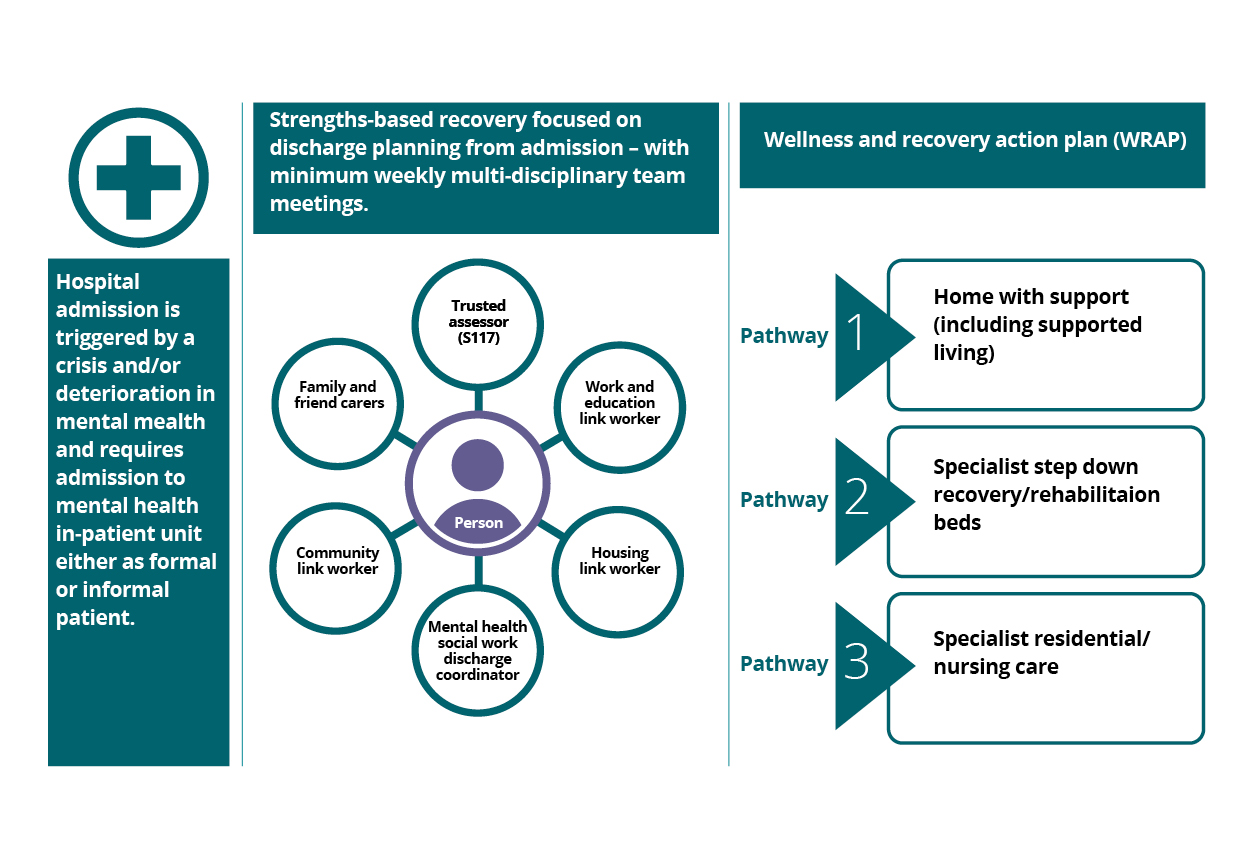
Hospital admission
Hospital admission is triggered by a crisis and/or deterioriation in mental health and requires admission to mental health in-patient unit either as formal or informal patient.
Strengths-based recovery
Strengths-based, recovery focused on discharge planning from admission with minimum weekly multi-disciplinary team meetings.
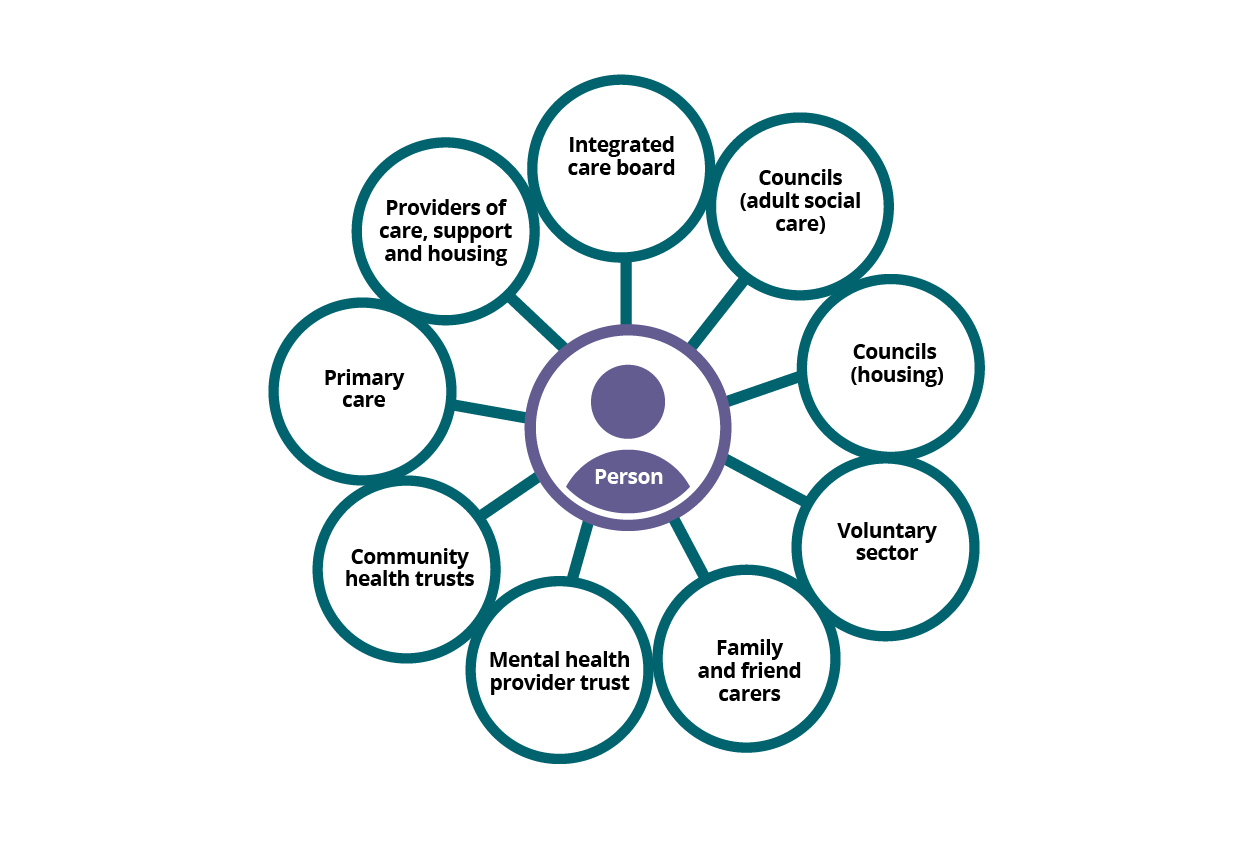
The key system partners essential to ensuring excellence in discharge from mental health settings are integrated care board, councils (adult social care), councils (housing), voluntary sector, family, friends and carers, mental health provider trust, community health trust, primary care, and providers of care, support and housing.
Wellness and recovery action plan (WRAP)
Pathway 1 - Home with support (including supported living)
Pathway 2 - Specialist step-down recovery or rehabilitation beds
Pathway 3 - Specialist residential or nursing care.
Essential system partnerships
Why is this important?
Having correct system partners is essential to ensure excellence in discharge from mental health settings for the following reasons."
In summary, having the correct system partners ensures a coordinated, comprehensive, and person-centred approach to discharge planning from mental health settings. This collaboration at a strategic and operational level is crucial for addressing the multifaceted needs of the person, promoting mental health recovery, and enhancing overall mental health outcomes.
Summary of organisational roles:
Key priorities and activities
To achieve excellence in discharge for the person, the following are essential to successful system partnership working:
- system partners focus on outcomes for the person not organisational boundaries
- discharge services are designed in partnership with people with lived experience/carers and local VCSFE organisations
- there are locally agreed protocols in place, and which are regularly reviewed which set out:
- roles and responsibilities and timescales for responding.
- arrangements for funding (Section 117 and Continuing Health Care (CHC))
- strengths–based risk management
- joint commissioning arrangements that provide access to high quality rehabilitation, recovery, and enablement support for positive mental health
- dedicated mental health social work discharge coordinator(s) to work as part of the multi-disciplinary team undertaking statutory Care Act functions and focusing on strengths-based, recovery focused, outcomes. This also requires close liaison between the mental health provider and council for services within a section 75 and robust joint working when councils directly deliver services.
- access to housing and supported living to support timely discharge.
- a clear, joint commitment to services that support prevention, rehabilitation, recovery, and enablement
- clear links to care transfer hubs (or equivalent) to enable people with physical health needs (as well as mental health needs) to access local discharge to assess services
- clear arrangement for identifying Continuing Health Care (CHC) responsibilities and providing bridging arrangements to support discharge prior to determination of CHC eligibility if required
- agreed arrangements for undertaking Section 117 duties, ideally considering options for trusted assessment to enable a single joint assessment
- multi-agency discharge events (MADE) can be used to bring partners together to systematically support safe and timely discharge, identifying good practice and unblocking challenges.
Frameworks
Why is this important?
Achieving excellence in person centred discharge from inpatient mental health settings requires colleagues to have a good understanding of both the legal and practice frameworks that need to be considered. These relate both to the process of discharge planning and the statutory considerations that are specific to the Mental Health Act.
Legal framework – Section 117
Section 117 After Care, Mental Health Act
Section 117 of the Mental Health Act 1983 (as amended, 2007) places a legal obligation on NHS and councils to provide after care for people who have been detained under certain qualifying sections of the Mental Health Act. Its core aim is to guarantee support and services to people after being discharged to try to avoid or minimise the person being readmitted to hospital.
Section 117 applies to:
Section 3 (admission for treatment)
Section 37 (‘hospital order’) – includes s.37/41
Section 45A (where a criminal court imposes a prison sentence but directs, they start their sentence in a psychiatric hospital for treatment)
Sections 47 and 48 (the transfer of prisoners to hospital)
Includes those on leave (s17) who have left the hospital to live somewhere else (but not for purposes of escorted day trips into the community)
Those subject to Community Treatment Orders (CTOs)
Section 117 does not apply to
People detained in hospital for assessment under Section 2
People detained in an emergency under Section 4
People detained while already in hospital under Section 5(2)
People who were not detained under any formal MH Act section (informal patients)
Although the statutory duty of Section 117 is triggered when the patient “ceases to be detained and (whether or not immediately after so ceasing) leaves hospital.
(Section 117(1)), Section 117 assessments should commence on the day of admission. The Mental Health Act Code of Practice states that:
Although the duty to provide after-care sevices begins when a person leaves hospital, the planning of after-care needs to start as soon as the patient is admitted to hospital. CCGs (ICBs) and local authorities should take reasonable steps, in consultation with the care programme approach care co-ordinator and other memebers of te multi-disciplinary team to identify appropriate after-care services for patients in good time for their eventual discharge from hospital or prison."(CoP 33.10)
A Section 117 assessment should be coproduced with the person and their carer, family and or representative and a range of professionals. The purpose of the assessment is to (Eligibility Criteria Section 117 (6) Mental Health Act):
- identify what needs the person has either arising from or related to the persons mental disorder. This includes any type of mental disorder the person suffers from, not just the one which caused their detention (for example, if a person develops dementia following discharge, the need arising from or related to dementia would also be included under Section 117).
- consider after care interventions, services or support to reduce the risk of a deterioration of the person’s mental condition (and accordingly, reducing the risk of the person requiring admission to a hospital again for treatment for mental disorder).
With regards to Section 117 there is a positive objective to prevent deterioration, not just to prevent readmission due to a particular disorder.
[Note: Councils cannot fund health services and will focus on social care needs including those needs which, while not falling within Section 117 (6) may fall within the scope of the Care Act, for example, physical disabilities.]
Section 117 and mental capacity
Section 117 After Care assessments should take account of the person’s mental capacity to engage in them. If a person lacks the capacity to consent to treatment, accommodation, and so on, decisions about their after care should be based upon their best interests in accordance with the Mental Capacity Act (2005), taking account of their preferences, views of carers, less restrictive options, and so on. Note: they do not have to give consent to the after care package, it is not what they want but what they need.
Section 117 after care assessments and advocacy
Those whose Section 117 after care needs are being assessed while they are detained in hospital and those on a community treatment order have a legal right to an independent mental health advocate (IMHA). Assessors may need to involve an independent mental capacity advocate (IMCA) if long-term placement decisions are being made and the person lacks the capacity to make such decisions and where there is no person to consult on best interests (see Mental Capacity Act 2005).
Frameworks to support excellence in discharge planning
Acute inpatient mental health care for adults and older adults
The acute inpatient mental health care for adults and older adults published in July 2023 and updated in October 2023 provides a range of focused activities that should be completed within 72 hours of admission to reduce the time a person spends in hospital. This should include the completion of a holistic assessment, ensuring strength-based care planning is in place (this includes Section 117 assessments).
Culture of care standards for mental health inpatient services
The culture of care standards for mental health inpatient support was published in April 2024 and updated in June 2024. This is specifically focused on improving the experience of people with learning disabilities and autism. The standards aim to foster a positive culture in mental health inpatient services where. The twelve core commitments focus on:
- the lived experience of the person
- ensuring safety
- valuing relationships
- ensuring positive staff support
- equality, inclusivity and recognising differences
- avoiding harm
- needs led
- choice
- positive environments - that are inclusive and accessible and sensory and trauma appropriate
- things to do
- therapeutic support
- transparency
Care and treatment reviews
Care and treatment reviews (CTRs) are for people with learning disabilities and or autism who are at risk of or have been admitted to a mental health inpatient setting.
CTRs aim to reduce the amount of time people spend in hospital and bring people together to help to sort out any problems which can keep people in hospital longer than necessary. They do this by helping to improve current and future care planning, including plans for leaving hospital.
Red and green days
Red and green days is a framework that has been developed to ensure that no days are wasted whilst a person is in hospital. It is based on introducing daily multi-disciplinary meetings which focus on the person’s care plans, making sure the right interventions (for example, therapy, medication reviews and so on) are being enacted to move their care on every day (green days) rather than wasted days in hospital waiting for interventions (red days).
Discharge to assess
Discharge to assess (D2A) is a hospital discharge approach designed to ensure that long term assessments of need take place in the most appropriate environment, ideally the persons own home. It improves the efficiency and effectiveness of hospital discharge processes for patients who no longer require acute care but still need ongoing assessment and support. While initially developed with a focus on discharge from acute hospital settings, the principles and approach are equally applicable to mental health settings (noting that if applicable, Section 117 assessments and wellness, recovery, action plans (WRAP) should be completed prior to discharge and must specify D2A outcomes.)
Section 117 assessments and wellness recovery action plans must be completed prior to discharge. Depending on local arrangements Care Act Assessments or Continuing Health Care assessments can be done through a discharge to assess arrangement if appropriate. The timescales and arrangements for these assessments must be set out in the plan.
At its core, D2A enables a person to be discharged from hospital as soon as they are medically fit to leave, with their assessments and ongoing care needs being determined in a more suitable environment, typically their own homes or a community setting.
Discharge to assess services are provided free at the point of delivery and can be delivered in a person’s home or in a bed-based setting. They are designed to be short term and should be focused on rehabilitation, reablement or enablement, and recovery. The rationale is that this enables a more accurate assessment of any ongoing care and support needs in their usual living environment, while freeing up hospital beds for patients who need acute care.
Where D2A is enacted, follow up and assessments should be carried out with the person by the community mental health team in collaboration with the council mental health social care team (if not an integrated system) at the earliest opportunity and within a maximum of 72 hours of discharge, to ensure the right discharge support is in place.
Mental health recovery model
The mental health recovery model is a holistic, person-centred approach to mental health care that focuses on empowering individuals with mental health conditions to lead meaningful and satisfying lives. It emphasises recovery as a personal journey rather than merely the alleviation of symptoms.
The mental health recovery model represents a shift from traditional, deficit-based approaches to one that emphasises hope, empowerment, and the potential for individuals to lead fulfilling lives despite the challenges of mental health conditions.
The key focus of the model is to:
- building resilience to cope with the challenges of mental illness.
- validating personal experience
- improving quality of life
- cultivating strategies and ensuring access to support for when challenges do arise and always aiming to do ‘with’ people rather than ‘to’ or ‘for’ people.
- focusing on what people can do rather than what they cannot do
- supporting people to develop skills to help themselves stay well
- working with the whole person and not just their diagnosis.
Wellness Recovery Action Plan (WRAP)
WRAPs are a tool that can aid a person’s recovery by providing a framework to monitor wellness, times of being less well and times when experiences may be uncomfortable and distressing. When developed with the person it will detail how they would like others to support them at these various times.
There are five key concepts that are at the core of WRAP:
- hope: the belief that we can get well, stay well, and go on to fulfil our dreams and goals.
- personal responsibility: It is up to each of us to act and do what needs to be done to stay well.
- education: learning all we can about what we are experiencing helps us make good decisions about all parts of our lives.
- self-advocacy: reaching out to others and expressing our needs helps us get what we need, want, and deserve to support our wellness and recovery.
- support: receiving support from others, and giving support, will help us feel better and enhance our quality of life.
Local systems may develop different styles of WRAP; however, they would normally cover: things that keep me well; things that I find stressful; early warning signs; becoming unwell; crisis plan; post crisis plan.
Discharge pathways
Why is this so important?
Discharge planning should start at the point of admission, with development of a holistic strengths-based recovery plan, clarity on the in-patient treatment and the likely medium to longer term community support requirements.
Summary of key actions required within the first 72 hours following admission to support discharge
People, families and relevant professionals should be given 48 hours notice of a decision to discharge
A risk assessment must be completed in collaboration with the patient
A follow-up meeting arranged (72 hours after discharge)
Information for people or families on crisis support
Discharge plans shared with person, carer and relevant professionals, including GP
There should be regular (minimum of weekly) multi-disciplinary (MDT) meetings involving the person or advocate, family and or friend carers and other relevant professionals to review the plan. The MDT should include those who are involved both in enacting the inpatient treatment plan, and support after discharge. For people with learning disabilities and autism the MDT should include a person's care and treatment review (CTR), as appropriate.
Trusted assessor (section 117)
Professional trusted to undertake section 117 assessment on behalf of NHS and council.
Work and education link worker
Usually a professional voluntary sector organisation(s) who can support with engagement in new or existing work or education activities.
Mental health housing link worker
Professional who can support with identifying and solving housing and tenancy issues.
Mental health social work discharge coordinator
Professional to undertake an assessment in response to the appearance of need of need as defined by the Care Act for the person (section 9) or the carer (section 10).
Mental health community link worker
What local community assets are in place that can support on discharge, services, social activities, therapeutic and well-being activities, technology or digital support. Any employment support needed?
Peer support worker
Peers are people who have lived experience of mental health challenges themselves. They use these experiences and empathy to support other people and their families receiving mental health services. Peer support workers join other members of someone’s care team to help support their wellbeing and provide inspiration for their recovery.
Family, friends, and carers
Individuals who provide unpaid care and support for the person.
These meetings should consider:
- the person: What is important to me and how can I support my discharge?
- the inpatient team: What do we need to be doing to help achieve timely discharge?
- the community team: What do we need to put in place to support safe and timely discharge on ongoing support?
Clinically ready for discharge (CRFD): NHS England defines the point at which someone is CRFD is reached when the MDT conclude that the person does not require any further assessments, interventions and/or treatments, which can only be provided in an inpatient setting.
There are three key criteria, which need to be met, before the MDT can make this decision:
- there must be a clear plan for the ongoing care and support that the person requires after discharge, which covers their pharmacological, psychological, physical health, social, cultural, housing and financial needs, and any other individual needs or wishes
- the MDT must have explicitly considered the person and their chosen carer/s’ views and needs about discharge and involved them in co-developing a discharge plan
- the MDT must have involved any services external to the provider in their decision-making, where these services will play a key role in the person’s ongoing care, for example, social care teams and housing teams.
As part of the discharge planning processes, the following should be in place at least 48 hours prior to a person’s discharge from a mental health setting:
- the person, families, and relevant professionals (for example, housing, community teams, adult social care and so on) should be given notice of a decision to discharge
- a risk assessment must be completed in collaboration with the person and those involved in their care and support in the community
- where temporary/short term accommodation is proposed, a clear rationale and exit route should be in place and shared
- completion of the WRAP which would have been coproduced with the person and those involved in their care and support in the community
- the WRAP and risk assessment should be shared with the person, carer and relevant professionals including GP
- a follow up meeting arranged (72 hours post-discharge) with the person and relevant mental health professional/s (may be joint visit with health and social care and so on).
Summary of key actions to take prior to discharge
The three discharge pathways
The discharge to assess model (D2A) is based around three discharge pathways
Pathway one
The aim should be for a person to return home or to their usual place of residence on discharge, with appropriate support in place promptly. This can equally apply to a person leaving hospital with a Section 117 after care plan, or with the intention of an assessment by the NHS or social care in the community (D2A). If a person needs access to physical health as well as mental health services, then they should be able to access locally commissioned rehabilitation, reablement or enablement, and recovery services at home.
Pathway one discharges will be appropriate for people who will draw on community mental health recovery support, tenancy, and housing support, supported living, packages of care and support including direct payments, enhanced GP or primary care support, rehabilitation or enablement support for mental health including work and education. It also includes short term support provided within a supported living / housing scheme that is not a registered residential home. For physical health needs there should be easy access to acute rehabilitation, reablement and recovery (3R) resources. Where temporary accommodation is the best available option, there should be a clear rationale and the plan to enable them to return to their own accommodation.
Pathway two
Pathway two is appropriate where a person needs a continuation of intensive support that is over and above what can be provided in the community. This may be a period of step-down rehabilitation or recovery with a view to supporting the person to return home after a further period on intervention(s). Pathway two beds can be hospital beds or registered nursing or care home facilities. The key is that they are a time limited intervention with a view to the person returning home. If longer term care and support in a bedded setting is likely to be needed this will be another move for the person.
If a person needs access to physical health as well as mental health then they should be able to access locally commissioned bed-based rehabilitation, reablement and recovery services.
Pathway three
Pathway three is appropriate where a person is unlikely to be able to be supported at home even with support. Pathway three beds are therefore generally only for people who are unlikely to recover sufficiently to enable them to return home (or who are already in nursing or residential care prior to admission) however it does not mean they cannot return home, but they should not be expected to move again if long term care is required.
Pathway three provision is likely to include a range of residential and or nursing support particularly dementia support, extreme self-neglect linked to mental health, Korsakoff syndrome, specialist learning disability or autism services.
References
- Hospital discharge and community support guidance (GOV.UK)
- Survey highlights mental health discharge planning problems (Community Care)
- Going lean in the NHS (NHSE)
- Social care and mental health: ending out of area placements (Centre for Mental Health)
- Acute inpatient mental health care for adults and older adults (NHSE)
- Mental Health, Learning Disability and Autism Inpatient Quality Transformation programme (NHSE)
- Supporting children and young people (CYP) with mental health needs in acute paediatric settings: A framework for systems
- What Is WRAP? - Wellness Recovery Action Plan
- PR1889-Safe-and-wellbeing-review-thematic-review-and-lessons-learned.pdf (NHSE)
- MCA: Care planning, involvement and person-centred care (SCIE)
- Introduction to Person-centred Planning Tools (NDTi)
- Promoting the health and wellbeing of looked after children (Department for Education and Department for Health, March 2015)
- Personalised care and support planning: a brief summary guid (NHSE)
- What is Personalised Care? The Comprehensive Model and the Six Components (Happy Healthy Lives)
- Strengths-based approach: Practice Framework and Practice Handbook (Department of Health and Social Care, February 2019)
- MHA_Code_of_Practice.PDF (publishing.service.gov.uk)
- Mental Health Act 1983 (legislation.gov.uk)
- Part 1: introducing recovery, peer support and lived experience initiatives - GOV.UK (www.gov.uk)
- Recovery Star™ | Recovery Model in Mental Health | Triangle (outcomesstar.org.uk)
- NHS England Care (education) and treatment reviews
- NHS England's Culture of care standards for mental health inpatient services